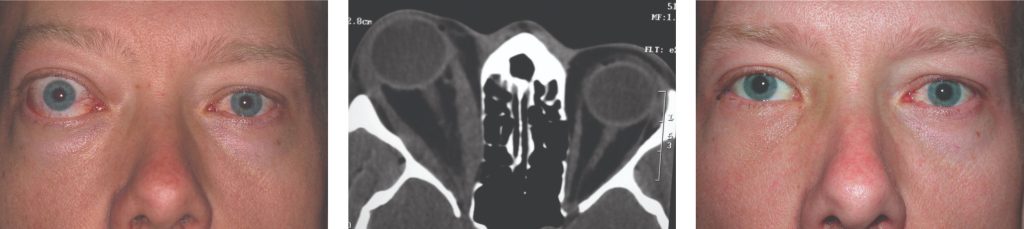
Optic nerve apical compression (DON) by expanded EOM is relieved by out-fracture of the medial orbital wall into the posterior ethmoid sinus and the medial floor into the maxillary sinus (Fig: Coronal CT showing LE apical crowding pre and post medial wall decompression). Even significant or longstanding vision loss may be reversed by an effective decompression. Adjunctive CS or RT may be offered to avoid postoperative deterioration in vision because of active disease with progressive muscle expansion.48
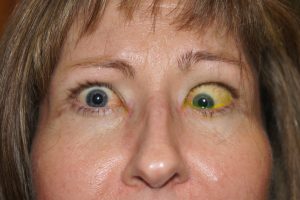
Proptosis reduction during the inactive phase is the most common indication, to improve comfort and appearance (Fig. Top shows RE proptosis and lid retraction; centre shows enlarged EOM and fat; bottom post decompression and lid narrowing). A swinging eyelid approach allows access to the lateral wall, floor, and medial wall, and any combination of bone wall removal and fat removal may be chosen, depending on the relative contribution of fat versus muscle tissue expansion. Specific complications are associated with each of the walls removed. Cheek numbness and globe inferior displacement may occur with floor decompression, oscillopsia may occur with lateral rectus/temporalis muscle apposition following lateral wall decompression,53 and sinusitis and ethmoidal nerve anesthesia may arise following medial wall decompression.
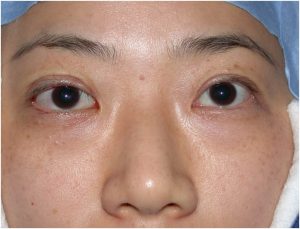
Reduction of long-standing orbital congestion is a rare indication. These individuals may have high CAS/VISA inflammatory scores, but the disease is inactive (false positive CAS) with stable VISA severity grades and poor response to GC. Improved venous drainage following surgery often results in a gratifying and immediate improvement in CAS/VISA I scores (Fig. shows inactive congestion on left and improvement after decompression on right, CLICK to enlarge).
RE Proptosis before and after decompression